


Neal-ing to Synthetics
Medical Marijuana Memory Blog #40

This past May marked the 45th anniversary of a little-known milestone in medical cannabis history. The first congressional hearing on medical cannabis in the modern era was held. It was called by the Task Force on Therapeutic Uses of Marihuana and Schedule I Drugs. Representative Stephen L. Neal, a Democrat from North Carolina, chaired it.
At that time, I was working at NORML, heading up the Medical Reclassification Project. I received a call from Robert M. Hundley, the chief of staff for the Task Force, who requested my assistance in identifying potential witnesses for the upcoming hearing. He explained that the committee was especially interested in cancer patients who could testify to the medical utility of cannabis.
By 1980, the use of cannabis in treating the side effects of cancer chemotherapy was well known, and, at the time, it was the primary force behind the medical cannabis movement. Cancer chemotherapy treatments of that time were brutal. Doctors freely admitted that they administered medicines that were more like poisons and hoped they could kill the cancer before the body. They often failed.
At the urging of a cancer patient, in early 1978, New Mexico became the first state to enact a law that recognized marijuana’s medical utility and established a program of legal access. Once New Mexico passed its law, cancer patients, or their loved ones, began lobbying in nearly every state. By the time of Hundley’s phone call, April 17, 1980, 25 states had passed laws authorizing state programs of legal, medical access to marijuana for victims of cancer and glaucoma. A feat that was all the more remarkable considering those laws had passed in just 26 months!
Cancer patients had emerged from every corner of the country with compelling stories that would break hearts and pass laws. We could have filled the hearing room with cancer patients supporting medical cannabis. But when Robert Hundley asked for a cancer patient to speak before the task force, my immediate thought —and reply—was Anne Guttentag.
Anne was a 49-year-old businesswoman, operating a doll shop in New Hope, PA. Her husband was a law professor at nearby Trenton State College (now the College of New Jersey). In 1976, Anne was diagnosed with breast cancer. With a radical mastectomy and chemotherapy, Anne thought she had beaten the devil. But the cancer returned in early 1979, this time in her ovaries, and the treatment with cisplatin and adriamycin was brutal. After her first treatment, she experienced 16 straight hours of nausea, vomiting, and convulsive dry heaves. None of the prescribed medicines helped with the side effects. She was encouraged to try marijuana and, to her amazement, it helped a lot. But Anne didn’t like breaking the law, so she began seeking legal access, and she asked her doctor to get her legal marijuana. He agreed, but how? Anne didn’t know, so she contacted a local reporter to share her story. His article was forwarded to me at the Medical Reclassification Project, and I immediately contacted her. That was in early April 1979.
Since Pennsylvania had not yet passed a law, Anne’s only option was a Compassionate IND (Investigational New Drug application). My late husband, Robert Randall, had become familiar with the complicated paperwork that was required, and he agreed to work with Anne’s doctor to craft her request. About six weeks after we first made contact, in May 1979, Anne’s doctor filed her Compassionate IND request with the FDA. It all seemed so reasonable. Anne was confident she would soon have federal marijuana. We weren’t so sure.
Anne waited for five months. Finally, in November 1979, just in time for her final scheduled chemotherapy session, THC pills arrived. FDA insisted she try the synthetic pills. They failed miserably. In January 1980, she was back for more chemo after tests showed the cancer was rebounding. Again, she tried the THC and it failed. FDA insisted she try the THC pill six times. She even agreed to give up her illegal marijuana. When, at last, the government agreed to send the marijuana cigarettes, it would be in time for her chemo in June, right after the Neal Hearing.
The Crash of Nabilone
To understand how we arrived at the Neal Hearing, a brief backstory is necessary. As the medical marijuana movement gained momentum in the late 1970s, federal officials initially weren’t concerned. They had an ace up their sleeve: Nabilone. Chemically, the synthetic Eli Lilly drug was a kind of first cousin to delta-9 THC. Nabilone was not derived from the cannabis plant, although Eli Lilly did have a long and respectable run as a medical cannabis manufacturer in the first part of the 20th century. Precisely when nabilone was developed is somewhat unclear. One researcher who joined Eli Lilly in 1971 recalled talk of Nabilone at that time. (Nahas, 1999) So, possibly, it dates back to the late 1960s or even earlier. It may have emerged in the murky days of MKULTRA.
Whatever its origin, it was the Great White Hope of federal drug agencies in the late 1970s. It was being tested as an anti-emetic, particularly for cancer patients, and the results were good. As more and more states passed marijuana-as-medicine laws, federal bureaucrats were confident that Nabilone could save the prohibition. One 1978 headline spelled it out, “Nabilone steals march on pot as medicine” (1978). The government even began floating stories about Nabilone’s promise before its approval, a rather shocking breach of FDA protocol, which prohibits the promotion of a new drug before final approval

But Nabilone would not save the federal government from medical cannabis. In June 1979, as Anne Guttentag was grinding her way through chemotherapy treatments and hoping to soon have legal marijuana, Eli Lilly publicly reported that beagle dogs in long-term research studies of Nabilone had experienced seizures and died. Despite some public pressure on Eli Lilly to continue research, the pharmaceutical giant chose to stop all tests and return to the drawing board.
Enter the National Cancer Institute
The withdrawal of Nabilone was a catastrophe for federal drug agencies. Pressure was building to cooperate with the 25 state marijuana-as-medicine programs, and the federal bureaucrats had to do something. They turned to synthetic delta-9 THC, which had been used in some research studies involving cancer patients but was erratic in its formulation. It was designed for animal research and never intended for regular human use. Never mind, trying times sometimes demand overlooking the specifics.
FDA turned to the National Cancer Institute for help. NCI agreed, although not with a lot of enthusiasm. It listed delta-9 THC as part of its Group B program, a means for researchers and clinicians to participate in research on promising anti-cancer drugs in the FDA pipeline. In 1979, the FDA began encouraging states and individual physicians to participate in Group B with delta-9 THC, but, according to the NCI representative at the Neal hearing, despite “numerous inquiries,. . . few actually filed protocols.” He attributed the lack of participation to marijuana’s Schedule I classification and the need for physicians to individually file for a permit from the DEA.
Now, NCI was upping the ante. At the Neal Hearing, it announced it was releasing delta-9 THC via its Group C program, which was far more accommodating than Group B. This move, according to the NCI representative, meant the “compound is considered to have documented medical efficacy for a specific indication” (Therapeutic Uses of Marihuana and Schedule I Drugs, p. 162). In and of itself, this was a monumental admission in 1980. Movement to Group C would make the drug available through regional, community, and medical school hospitals affiliated with the Group C program, which encompassed nearly every hospital with an oncology department. It eliminated the need for physicians to apply individually to the DEA for a special license. Essentially, the move was making this still-investigational drug available by prescription, with minimal additional work required for the physician. It was an enormous escalation.
It was a bombshell of an announcement. Medical cannabis advocates, like myself, were caught flat-footed. NCI’s researchers had been openly critical about the poor formulation of THC, and we never anticipated the agency would promote public release of the drug. In hindsight, it was the only option for federal drug agencies who were intent on keeping natural cannabis under tight control, and the congressional setting offered a controlled environment in which to drop the news of this mammoth change in federal policy.
A month later, on June 26, 1980, the FDA’s oncologic advisory committee narrowly approved the release of delta-9 THC through Group C. The tie vote was broken by the committee’s chair, Dr. Philip S. Schein, who testified at the Neal Hearing and supported the Group C release.
Meanwhile, Anne Guttentag was still waiting for her legal marijuana. It was not available at her June 6th chemotherapy session, even though it had been promised. On June 9th, she wrote Rep. Neal a letter,
“I was treated again on June 6 with only the pills (THC) and Compazine. Needless to say both failed. I am about ready to give up. The fight to live is not worth going through this anymore. I feel no one cares, nor will anyone do anything to help. … Where is the group who told your committee that there was no problem with the paperwork and that the marijuana was now easy to get? Show them this letter, for someone is telling an untruth.” ( Pg 6)
The marijuana was available at Anne’s next session on July 24, 1980, thirteen months after asking for it, but just five weeks after her powerful letter to Rep. Neal. She called to tell me they made a “BIG difference.” Her voice was weary but triumphant. Anne Guttentag became the first woman to receive federal marijuana via the Compassionate IND program, but it would not save her. In her final months, she experienced a nightmare of medical and physical complications. She died on August 23, 1981.
March Out the Band
As Anne suffered in Pennsylvania, the government lost no time in announcing the news about Group C. As the program was rolled out, the federal drug agencies filled the news media with talk about this wonderful new pill that “is just like marijuana”. (1980)
Well, it wasn’t, of course. The government’s media blitzkrieg even claimed the THC was made from marijuana, which it wasn’t. We fired back with press releases of our own, sharing the news of NCI’s earlier reluctance to release delta-9 THC and noting that giving pills for vomiting might not be the best approach. (1980, November 22) But it was a done deal, and even though initial enrollment was slow, cancer patients were desperate and willing to give THC a try. The true rollout of Group C did not occur until late in 1980. By the end of 1982, NCI had distributed half a million THC capsules in 5mg and 2.5 mg doses. (Annual Report, 1985) This was the high-water mark for NCI's distribution of THC. Unimed, a small pharmaceutical company in New Jersey, assumed responsibility for THC after 1982.
Reflections
From this vantage point, 45 years later, I can still get angry when I think of the efforts of the FDA and NCI regarding Group C. It was a betrayal of cancer patients because the FDA knew inhaled marijuana was more effective. It admitted as much five months before the Neal Hearing in a news article on the Scripps-Howard News Service. The agency’s chief of drug abuse, Edward C. Tocus, stated that research had shown “marijuana cigarettes would prevent nausea in 90 percent of cancer patients, while the marijuana pills are effective only 60 percent of the time.” (Kirkman, 1980)
So, why were we releasing the inferior medicine? Why were we condemning people like Anne Guttentag to needless suffering, a “living hell” as she called it? Why was it so hard to get a simple weed?
But the flip side is that the FDA and NCI did get delta-9 THC out to the public. Perhaps 60% of those who would not have otherwise received relief did get it. In 1985, synthetic delta-9 THC would become dronabinol and then Marinol, its trade name, the first cannabinoid to be rescheduled and released to the public by prescription. (Joy & Watson) The federal government, particularly the Drug Enforcement Administration, never intended or wanted this. But pressure from patients and the many states that passed the marijuana-as-medicine laws, plus the untimely collapse of Nabilone, all came together in May 1980.
The Neal Hearing was a quiet and unassuming event, but it altered the medical cannabis landscape in the 1980s. The government succeeded in quelling the demand for medical cannabis... for a while. But in releasing THC, it had to pay a price. It was forced to reschedule a cannabinoid, thus cracking the absolute prohibition it had upheld for so many years. Ironically, the need to reschedule delta-9 THC put medical cannabis reformers in the catbird seat and led to a gigantic opportunity to create a factual and public record about medical cannabis in the 20th century. That will be the topic of our next Medical Marijuana Memory Blog. ❖
If you would like to know more about the Neal Hearing, Project 50 has scanned the hearing transcript, which is available on my website. With 300+ pages of witness testimony and submitted evidence, this document is a must-have for medical cannabis enthusiasts. And, it’s free!
Please sign up for my blog. It’s free. If you wish to support my efforts and Project 50, please visit my website at www.aliceolearyrandall.com. Sorry for the inconvenience. Substack’s credit card processor, Stripe, has refused my account because my blog mentions cannabis, and I sell historic cannabis memorabilia. The battle goes on, even in the 21st century.
_____
References
Therapeutic Uses of Marihuana and Schedule I Drugs, Hearing Before the Select Committee on Narcotics Abuse and Control, House of Representatives 96th Congress, Second Session, 1980.
Nahas, G. G. (1999). Marihuana and medicine. Spring+Business Media.
(1978, October 15). Nabilone steals march on pot as medicine [Review of Nabilone steals march on pot as medicine]. Fort Worth Star Telegram.
(1980, November 27). Government readies “pot pills” to ease chemotherapy effects [Review of Government readies “pot pills” to ease chemotherapy effects]. The Miami Herald.
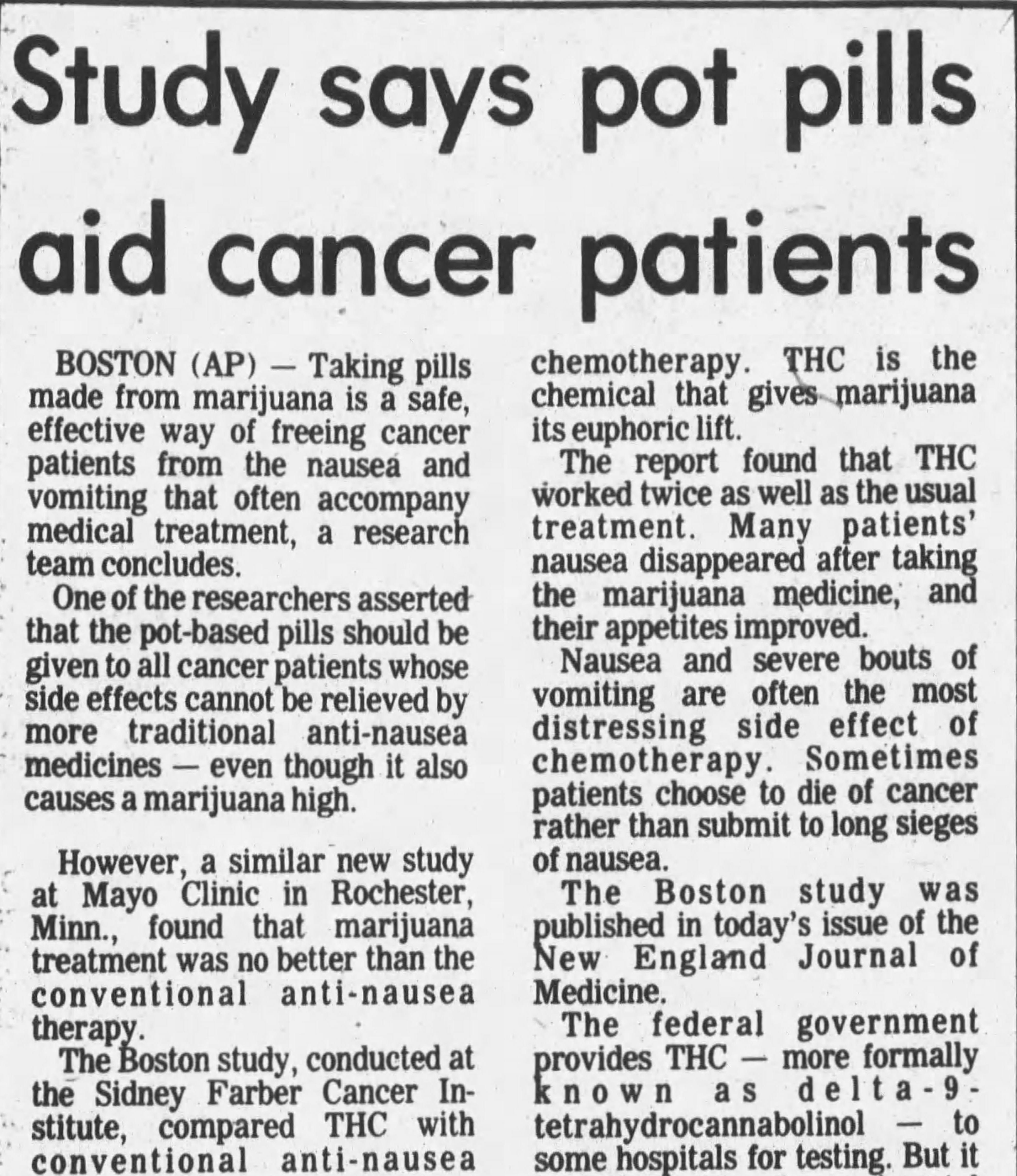
(1980, January 17). Study says pot pills aid cancer patients [Review of Study says pot pills aid cancer patients]. The Transcript (North Adams, MA).
(1980, November 22). The THC-vs.-pot debate [Review of The THC-vs.-pot debate]. The San Francisco Examiner.
(February 1985) Annual Report to the Food and Drug Administration Delta 9 THC, National Cancer Institute, March 1982, Alliance for Cannabis Therapeutics Freedom of Information request.
Medicine (US), I. of, Joy, J. E., Stanley J. Watson, J., & John A. Benson, J. (1999). Development of Cannabinoid Drugs. In www.ncbi.nlm.nih.gov. National Academies Press (US). https://www.ncbi.nlm.nih.gov/books/NBK230708/